
The Science
The Metrics Study - Our Research in Glioblastoma Stage-IV Brain Tumors
Care Oncology has conducted a preliminary internal analysis comprising 95 patients with a biopsy confirmed Glioblastoma IV brain tumor. Patients could be enrolled onto the adjunctive COC Protocol at any time i.e., from presentation of their GBM or at any future time-point if deemed eligible to receive treatment by the consulting COC clinician. All patients continued to receive their standard-of-care therapy and follow up.
The primary endpoint was overall survival (defined as time from diagnosis until death from any cause).
- Mean age was 53.7 years
- Majority of patients were male [65 patients (68.4%)].
- Median time from diagnosis to starting the adjunctive COC protocol was 6.64 months.
- Cohort (n = 95) had a median survival of 26.3 months and a two-year survival of 55. 8%
GBM cohorts receiving optimal standard of care alone:
Median survival of 14.8 months in the Public Health England dataset (Brodbelt et al., 2015) and 15.8 months in a study by the European Organisation for Research and Treatment of Cancer (Stupp et al., 2005), with a 2-year survival of 28.7% and 26.5%, respectively.
The open-access perspective article in Frontiers in Pharmacology can be found here
Further reading
Targeting cancer’s metabolic pathways
Metabolism is the conversion of food to energy to run cellular processes and construct cellular building blocks. It is widely accepted that the metabolism of cancer cells is usually fundamentally different compared to that of healthy non-cancerous cells. Altered metabolism is now considered a hallmark of cancer and a new discipline of “metabolic oncology” has emerged (Hanahan and Weinberg, 2000; Hanahan and Weinberg, 2011; Bergers and Fendt, 2021).
Cancer cells need large amount of energy to survive and grow. They commonly use an adaptive process called aerobic glycolysis (the ‘Warburg effect’) to generate the excessive energy they need (Kroemer and Pouyssegur, 2008; Liberti and Locasale, 2016).
The COC Protocol targets various molecular processes involved in and surrounding aerobic glycolysis and cancer metabolism, aiming to restrict cancer cell energy supply and use, while simultaneously preventing the cells from adapting and using other pathways to take up energy.
As a result of ongoing metabolic restriction, (Jang et al., 2013), cancer cells may become weaker and less able to take in and use nutrients they need from their surroundings (e.g., glucose, lipids, and essential amino acids such as glutamine and arginine). This may potentially make it more difficult overall for cancer cells to survive, grow, spread, and adapt to changing conditions in the body (Martinez-Outschoorn et al., 2017; Jagust et al., 2019).
Gradually, metabolically weakened cancer cells (including more resilient and previously treatment-resistant cells) can potentially become more vulnerable to attack from other cell‑killing cancer therapies such as radiotherapy, chemotherapy, and other therapies (Luo and Wicha, 2019; Zhao et al., 2013; Butler et al., 2013).
Why use a combination approach?
Cancer therapies may be most effective when used in combination. Review of peer-reviewed literature suggests that each individual element of the COC Protocol may target cancer cell metabolism in a distinct and potentially complementary way, and we have termed this action ‘mechanistic coherence’, which describes the possibility of attacking a cancer cell from different angles in a synergistic or additive fashion, and potentially offering greater benefit than the addition of one adjunctive therapeutic agent on its own. This type of combination approach in cancer is discussed by Mokhtari et al., 2017, and others.
Our drug selection criteria
Care Oncology scientists and clinician selected the COC Protocol medications from a huge number of potential candidates, following a detailed analysis of their biology and associated anticancer data.
Final selection was based on the strength of peer reviewed data in certain key areas, including:
- level of data in humans
- level of data in humans with cancer
- well-established and well-understood safety profiles for their approved indications
- low drug-drug interaction burden
- documented potential to target and slow down the growth of cancer
- predicted capacity to work together in a complementary way against cancer, and enhance the activity of standard-of-care treatments
Protocol mechanisms
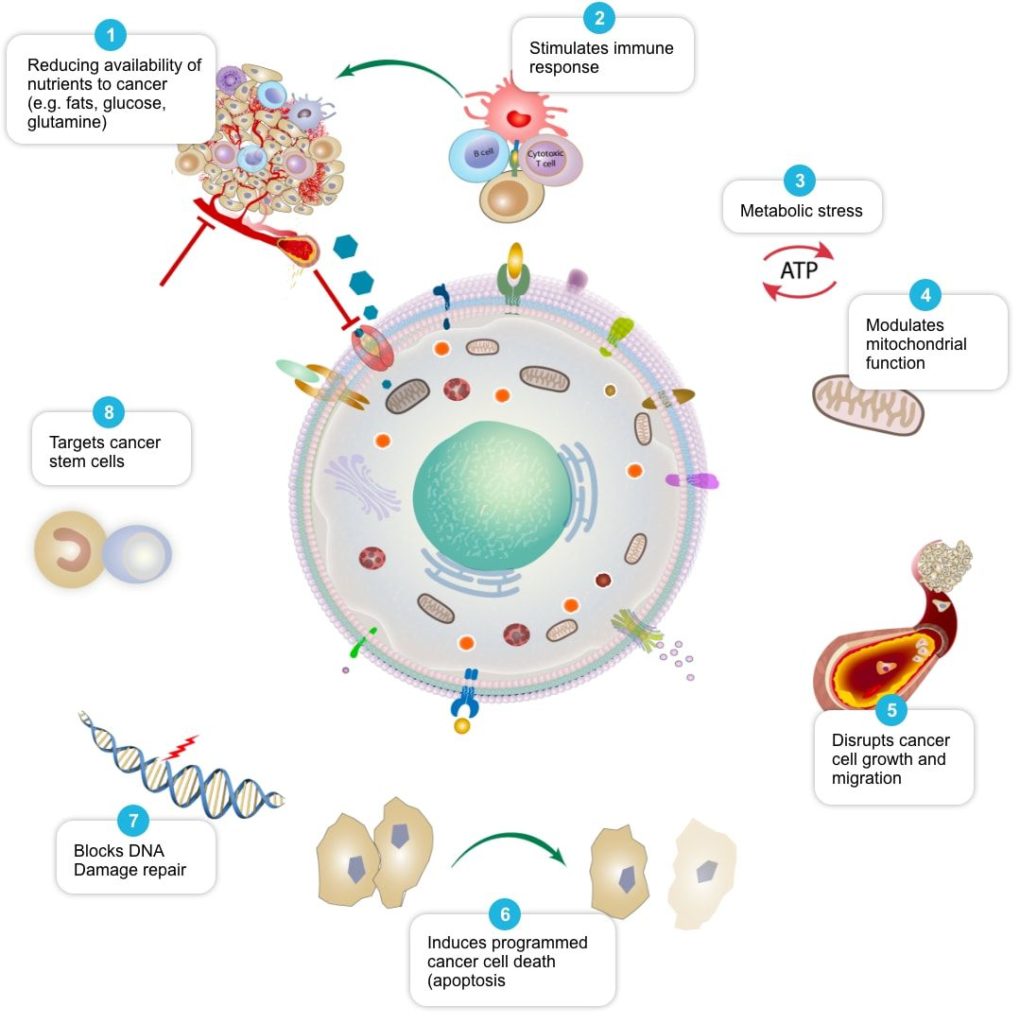
This graphic below shows some of the potential mechanisms of action for agents used in the COC Protocol as reported in the scientific literature. This is an evolving field of research, and this list is not exhaustive. Refer to the References table below for a list of relevant published papers.

The Science – Care Oncology USThe Science The Metrics Study – Our Research in Glioblastoma Stage-IV Brain Tumors Care Oncology has conducted a preliminary internal analysis comprising 95 patients with a biopsy confirmed Glioblastoma IV brain tumor. Patients could be enrolled onto the adjunctive COC Protocol at any time i.e., from presentation of their GBM or at any future time-point |
The Metabolism of Cancer
The COC Protocol was developed by Care Oncology Clinic (COC) in 2013 and is based upon the work of German scientist Otto Warburg, who received a Nobel prize for his research into cancer’s unique cellular biology.
Scientists unveil the secret of cancer-associated Warburg effect
Di Zhang, Zhanyun Tang, He Huang, Guolin Zhou, Chang Cui, Yejing Weng, Wenchao Liu, Sunjoo Kim, Sangkyu Lee, Mathew Perez-Neut, Jun Ding, Daniel Czyz, Rong Hu, Zhen Ye, Maomao He, Y. George Zheng, Howard A. Shuman, Lunzhi Dai, Bing Ren, Robert G. Roeder, Lev Becker & Yingming Zhao. Metabolic Regulation of Gene Expression by Histone Lactylation. Nature, 2019 DOI: 10.1038/s41586-019-1678-1
As tumors develop and cancer cells quickly multiply, this can subject them to a lack of oxygen and key nutrients. To support continued growth in such a challenging environment, cancer cells adapt and alter their metabolism (the ways in which they access and use energy). Cancer cells depend more heavily on alternative metabolic pathways to survive and multiply under the metabolically compromised conditions provided by the tumor microenvironment.
The COC Protocol is an individualized therapeutic approach which seeks to target multiple cancer pathways through pharmaceutical management, nutrition and other interventions that address altered cancer metabolism. The pharmaceutical agents that comprise the COC Protocol have been shown to disrupt several proteins or signalling pathways, which can impact upon cancer cells’ energy supply, with the effect of killing these cells, restricting multiplication, or reprogramming them to behave like healthy cells. In addition, there is evidence that the medicines used may increase cancer cells’ sensitivity to chemotherapy, radiotherapy, hormone therapy and immunotherapy. By using the medicines in combination, we may be able to target multiple biological pathways, thus creating a synergistic effect and potentially delivering greater benefit than via the addition of one adjunctive therapeutic agent on its own.
Inflammation and Metabolic Dysfunction in Cancer
While conventional cancer treatments (including surgery, radiotherapy, chemotherapy, hormone therapy, immunotherapy) are intended to target cancer cells in the here and now, at Care Oncology, we aim to address root causes which facilitated the development of cancer. Two of these root causes are chronic inflammation and metabolic dysfunction, and some of the standard-of-care therapies used to treat cancer may in fact make these issues worse, with increasing numbers of patients reporting cancer treatment-related toxicities.
Care Oncology’s COC Protocol seeks to measure and track fundamental parameters, which if optimized, may improve cancer outcomes, and mitigate risks from treatment related toxicities. We evaluate these specific parameters via specialist blood tests and questionnaires, enabling provision of actionable insights to our patients based on their personalized scores.
COC doctors carefully review patient data and make personalised, evidence-based recommendations to help drive improvements. This can include advice around diet and nutrition, stress, sleep, exercise, as well as the recommendation or prescription of a specific set of supplements with an excellent evidence-base in the cancer setting.
In addition, the COC Plus blood test data enables our clinical team to objectively assess the degree of metabolic control which may be being exercised by COC Protocol pharmaceuticals and to further refine the dosing of these over time.
Tackling Chronic Inflammation and Metabolic Dysfunction
Obesity, Diabetes, Chronic Inflammation and Insulin Resistance are known risk factors for the development of many cancers. Therefore, cancer patients at diagnosis may be at greater risk of already having or developing Metabolic Syndrome
Insulin Resistance
Insulin resistance is when cells in your muscles, fat, and liver don’t respond well to insulin and can’t use glucose from your blood for energy. To make up for it, your pancreas makes more insulin. Over time, your blood sugar levels go up.
Metabolic Syndrome
Metabolic syndrome is a group of risk factors that include abdominal fat, high blood pressure, high blood sugar, and unhealthy cholesterol levels. Treatment is focused on tackling each of these conditions. The goal is to cut your odds of blood vessel disease and heart disease, as well as diabetes.
Published Papers Referenced in Text
Hanahan and Weinberg, 2000 PMID: 10647931, Hanahan and Weinberg, 2011 PMID: 21376230,
Bergers and Fendt, 2021 PMID: 33462499, Kroemer and Pouyssegur, 2008 PMID: 18538731,
Liberti and Locasale, 2016 PMID: 26778478, Jang et al., 2013 PMID: 24091747,
Martinez-Outschoorn et al., 2017 PMID: 27141887, Jagust et al., 2019 PMID: 30967773,
Luo and Wicha, 2019 PMID: 30573183, Zhao et al., 2013 PMID: 23470539,
Butler et al., 2013 PMID: 23610447, Mokhtari et al., 2017 PMID: 28410237.
Additional References
This table is a summary of some of the potential mechanisms of action reported for agents used in the COC Protocol as reported in the scientific literature. This is an evolving field of research, and this list is not exhaustive.
| Intended Mechanism Of Action | Supporting Literature |
|---|---|
|
1. Reduce availability of nutrients to cancer cell |
Rosilio C. et al. 2014 PMID: 24462823, Babcook M.A. et al. 2016 PMID: 27441003 |
|
2. Stimulate and facilitate immune response to cancer cell |
Al Dujaily E. et al. 2020. PMID: 32190817, Yongjun Y. et al. 2013. PMID: 23707077, |
|
3. Place cancer cells under ‘metabolic stress’ |
Pernicova I. et al. 2014. PMID: 24393785, Clendening J.W. et al. 2012. PMID: 22310279, |
|
4. Modulate mitochondrial function in cancer cells |
Ozsvari B. et al. 2017 PMID: 29080556, Cazzaniga M. et al. 2015 PMID: 26605341, |
|
5. Disrupt cancer cell growth and migration |
Kamarudin M.N.A. 2019. PMID: 31831021, Jiang W. et al. 2021. PMID: 34303383, Mukhopadhyay T. 2002 PMID: 12231542, Pinto L.C. et al. 2015 PMID: 26315676, Yang B. et al. 2015 PMID: 26111245 |
|
6. Induce programmed cancer cell death (apoptosis) |
Song H. et al. 2014 PMID: 25502932, Doudican N. et al. 2008 PMID: 18667591, Sasaki J. et al. 2002 PMID: 12479701, Bayat N. et al. 2016 PMID: 27836464, Cafforio P. et al. 2005 PMID: 15705602, Fromigué O. et al. 2006 PMID: 16470222, Kalinsky K. et al. 2017PMID: 27305912, Jiang W. et al. 2021. PMID: 34303383 |
|
7. Block cancer cell DNA damage repair |
Efimova E.V. et al. 2018 PMID: 29030460, Lamb R. et al. 2015 PMID: 26087309, Peiris-Pagès M. et al. 2015 PMID: 26425660 |
|
Slow growth of tumor-feeding blood vessels (anti-angiogenic activity) |
Bai R.-Y. et al. 2015 PMID: 25253417, Orecchioni S. et al. 2015 PMID: 25196138, Qian W. et al. 2018 PMID: 30053447 |
|
8. Target cancer stem cells and may help make them more vulnerable to standard cancer treatments |
Saini et al. 2018. PMID: 29342230, Brown et al. 2020 PMID: 32369446, Hirsch H.A. et al. 2009. PMID: 19752085, Scatena C. et al. 2018 PMID: 30364293, Yang B. et al. 2015 PMID: 26111245, Bayat N. et al. 2016 PMID: 27836464, Kato S. et al. 2018 PMID: 29848667, Kodach L.L. et al. 2011 PMID: 21551187, Jiang W. et al. 2021. PMID: 34303383, Markowska A. et al. 2019 PMID: 31054863, |